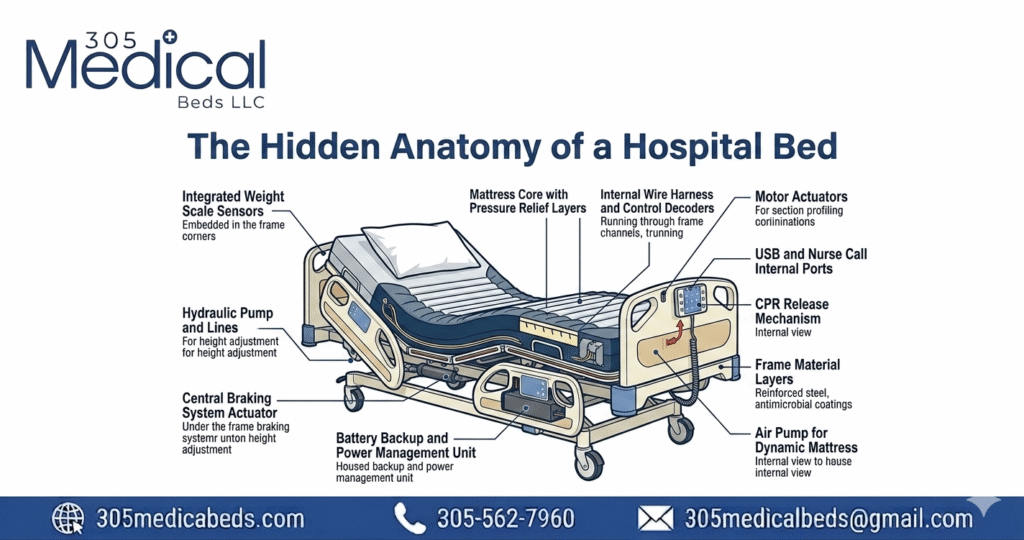
The Hidden Anatomy of a Hospital Bed — Every Part Explained
You’ve probably seen a hospital bed a hundred times — in a hospital room, at a rehab center, or in someone’s home. But have you ever looked at one and thought: what does each part actually do? Most people don’t. And that’s a problem — especially if you’re a caregiver setting one up at home, a patient learning to use one after surgery, or a family member trying to figure out why the bed suddenly won’t lower. The anatomy of a hospital bed is more thoughtful than it looks. Every single component — from the frame rails to the brake casters — was designed with one goal: keeping patients safe and caregivers in control. This guide breaks it all down, in plain language, so you know exactly what you’re working with. What’s covered in this guide Why Hospital Bed Anatomy Matters A hospital bed looks simple from the outside. But inside it is an engineered system with 15 to 30 individual components working together. Understanding those components matters for three very practical reasons: Whether you’re working with a basic manual bed or a full-electric model from a brand like Hill-Rom or Stryker, the core anatomy is largely the same. Let’s go through it part by part. 15-30 individual components per bed 04 adjustable deck sections 36″ standard bed width 80″ standard bed length The Bed Frame — The Structural Backbone Everything else on a hospital bed is attached to the frame. It is the skeleton of the entire system. Understanding the frame is the starting point for understanding everything else. What the Frame is Made of Hospital bed frames are almost always made from powder-coated steel — sometimes with aluminum alloy components in lighter-weight models. Steel is used because it can withstand the repeated stress of height changes, patient weight shifts, and years of daily use. The powder coating protects against rust, makes cleaning easier, and gives the frame its characteristic smooth, often white or silver finish. The Frame’s Three Sections Upper Frame Holds the deck and mattress The upper frame is the part you can see around the mattress. It holds the deck sections and connects to the head and foot boards. On electric beds, the upper frame also houses the motor mounting points. Lift Mechanism Controls height adjustment This is the scissor-jack or column mechanism that raises and lowers the bed’s overall height. On electric models it is driven by a motor; on manual beds, a crank at the foot of the frame drives it by hand. Base Frame Sits on the casters The base frame rests on the floor via the casters (wheels). It is the lowest, most structurally dense part of the bed — it bears all the weight and keeps the whole structure stable during patient transfers. Extension frame On length-adjustable models Some hospital beds — especially bariatric and extra-long models — have telescoping frame extensions that allow the bed’s overall length to be adjusted, accommodating taller patients without needing a completely different bed. Key frame fact for home buyers When comparing beds, check the frame’s weight capacity. Standard home hospital beds typically support 350–450 lbs. Bariatric models support 600–1,000 lbs. Always choose a frame capacity at least 50 lbs above the patient’s weight to account for movement forces during repositioning. If you’re choosing a hospital bed for home use, 305 Medical Beds carries both standard and bariatric frames — our team can help you match the right frame capacity to your situation. The Deck Sections — Where All The Positioning Happens The deck is the surface the mattress rests on. Unlike a regular bed, a hospital bed deck is not a single flat piece of wood or metal — it is divided into sections that can move independently of each other. This is what makes repositioning possible. The Four Standard Deck Sections Head section (backrest) Upper body elevation This is the largest and most-used section. It raises and lowers the patient’s upper body — from completely flat to as high as 75–80 degrees upright. This section is what helps patients with congestive heart failure breathe easier at night, lets post-surgical patients sit up without straining, and makes feeding or reading in bed possible. On electric beds, this section has its own dedicated motor. Seat section The fixed pivot point The seat section does not move — it is the fixed center of the deck, roughly where the patient’s hips sit. All the other sections pivot relative to the seat section. This design keeps the patient’s body centered on the bed even when the head and foot sections are raised, preventing the patient from sliding down or up as positions change. Thigh section Knee gatch — prevents sliding The thigh section is the short section between the seat and the calf. When raised, it creates a “knee break” — a gentle bend at the knees — that prevents the patient from sliding down when the head section is elevated. It is also called the “knee gatch” in clinical settings. This is a safety feature as much as a comfort one. Foot Section Leg elevation The foot section elevates the patient’s lower legs and feet. Raising this section reduces swelling (edema) by allowing fluid to drain back toward the body, helps manage varicose veins, and provides comfort for patients who cannot tolerate lying flat. On Trendelenburg-capable beds, the entire deck tilts so the feet are higher than the head — used in certain clinical procedures. Why the deck design matters for hip surgery patients: After hip replacement, surgeons require the hip to stay below 90 degrees of flexion. A hospital bed’s four-section deck allows the head to be raised without bending the hip — something a regular adjustable bed or recliner cannot safely do. This is one of the main clinical reasons a hospital bed is prescribed post-operatively. The Mattress — More Medical Than You Think A hospital bed mattress is not a regular mattress. It is a medical device in its own right. The wrong mattress on a hospital bed can cause pressure