You’ve probably seen a hospital bed a hundred times — in a hospital room, at a rehab center, or in someone’s home. But have you ever looked at one and thought: what does each part actually do?
Most people don’t. And that’s a problem — especially if you’re a caregiver setting one up at home, a patient learning to use one after surgery, or a family member trying to figure out why the bed suddenly won’t lower.
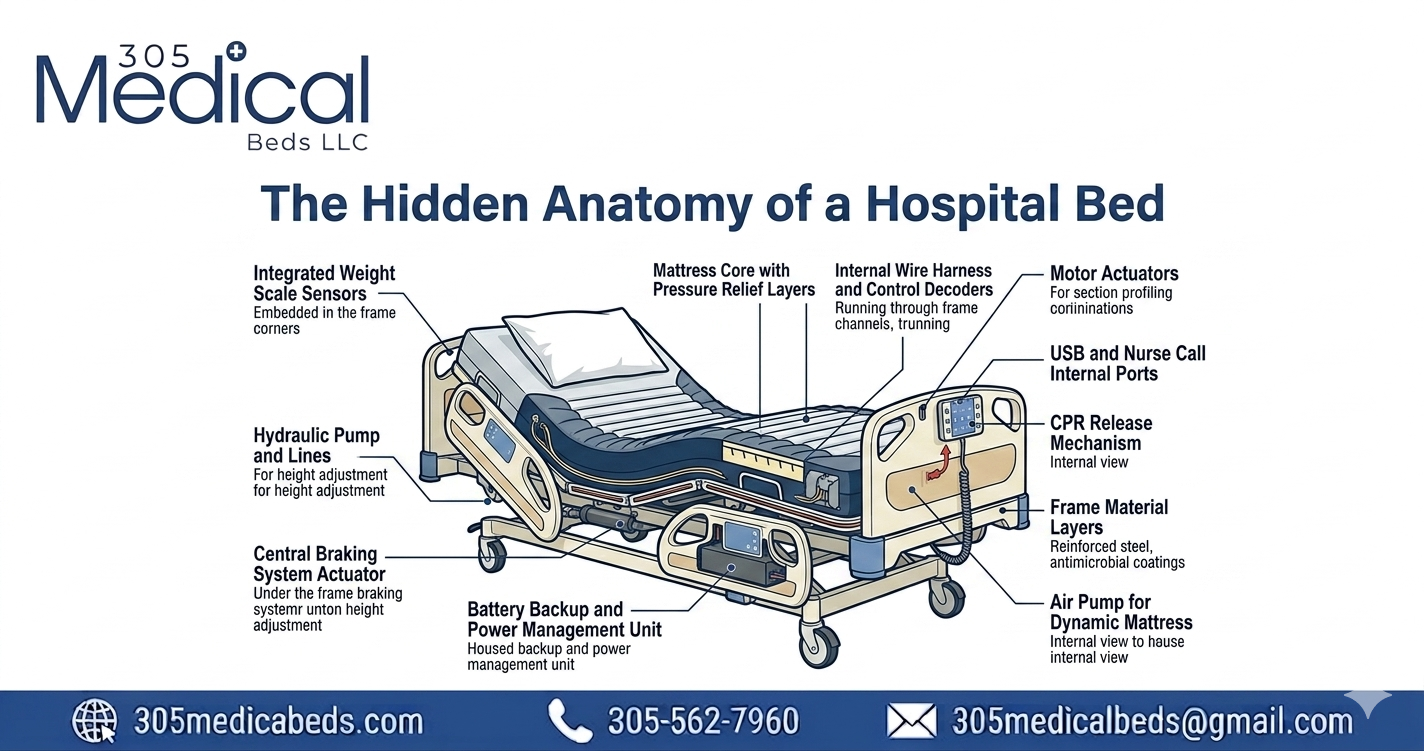
The anatomy of a hospital bed is more thoughtful than it looks. Every single component — from the frame rails to the brake casters — was designed with one goal: keeping patients safe and caregivers in control. This guide breaks it all down, in plain language, so you know exactly what you’re working with.
What’s covered in this guide
Why Hospital Bed Anatomy Matters
A hospital bed looks simple from the outside. But inside it is an engineered system with 15 to 30 individual components working together. Understanding those components matters for three very practical reasons:
- Safety: Knowing what each part does helps you use the bed correctly and avoid accidents — for both patients and caregivers.
- Troubleshooting: When something goes wrong (the bed won’t lower, the rails won’t lock), knowing the anatomy tells you where to look first.
- Buying decisions: When you’re comparing beds — for home use, a care facility, or insurance claims — knowing what features matter helps you choose the right one.
Whether you’re working with a basic manual bed or a full-electric model from a brand like Hill-Rom or Stryker, the core anatomy is largely the same. Let’s go through it part by part.
15-30
individual components per bed
04
adjustable deck sections
36″
standard bed width
80″
standard bed length
The Bed Frame — The Structural Backbone
Everything else on a hospital bed is attached to the frame. It is the skeleton of the entire system. Understanding the frame is the starting point for understanding everything else.
What the Frame is Made of
Hospital bed frames are almost always made from powder-coated steel — sometimes with aluminum alloy components in lighter-weight models. Steel is used because it can withstand the repeated stress of height changes, patient weight shifts, and years of daily use. The powder coating protects against rust, makes cleaning easier, and gives the frame its characteristic smooth, often white or silver finish.
The Frame’s Three Sections
Upper Frame
Holds the deck and mattress
The upper frame is the part you can see around the mattress. It holds the deck sections and connects to the head and foot boards. On electric beds, the upper frame also houses the motor mounting points.
Lift Mechanism
Controls height adjustment
This is the scissor-jack or column mechanism that raises and lowers the bed’s overall height. On electric models it is driven by a motor; on manual beds, a crank at the foot of the frame drives it by hand.
Base Frame
Sits on the casters
The base frame rests on the floor via the casters (wheels). It is the lowest, most structurally dense part of the bed — it bears all the weight and keeps the whole structure stable during patient transfers.
Extension frame
On length-adjustable models
Some hospital beds — especially bariatric and extra-long models — have telescoping frame extensions that allow the bed’s overall length to be adjusted, accommodating taller patients without needing a completely different bed.
Key frame fact for home buyers
When comparing beds, check the frame’s weight capacity. Standard home hospital beds typically support 350–450 lbs. Bariatric models support 600–1,000 lbs. Always choose a frame capacity at least 50 lbs above the patient’s weight to account for movement forces during repositioning.
If you’re choosing a hospital bed for home use, 305 Medical Beds carries both standard and bariatric frames — our team can help you match the right frame capacity to your situation.
The Deck Sections — Where All The Positioning Happens
The deck is the surface the mattress rests on. Unlike a regular bed, a hospital bed deck is not a single flat piece of wood or metal — it is divided into sections that can move independently of each other. This is what makes repositioning possible.
The Four Standard Deck Sections
Head section (backrest)
Upper body elevation
This is the largest and most-used section. It raises and lowers the patient’s upper body — from completely flat to as high as 75–80 degrees upright. This section is what helps patients with congestive heart failure breathe easier at night, lets post-surgical patients sit up without straining, and makes feeding or reading in bed possible. On electric beds, this section has its own dedicated motor.
Seat section
The fixed pivot point
The seat section does not move — it is the fixed center of the deck, roughly where the patient’s hips sit. All the other sections pivot relative to the seat section. This design keeps the patient’s body centered on the bed even when the head and foot sections are raised, preventing the patient from sliding down or up as positions change.
Thigh section
Knee gatch — prevents sliding
The thigh section is the short section between the seat and the calf. When raised, it creates a “knee break” — a gentle bend at the knees — that prevents the patient from sliding down when the head section is elevated. It is also called the “knee gatch” in clinical settings. This is a safety feature as much as a comfort one.
Foot Section
Leg elevation
The foot section elevates the patient’s lower legs and feet. Raising this section reduces swelling (edema) by allowing fluid to drain back toward the body, helps manage varicose veins, and provides comfort for patients who cannot tolerate lying flat. On Trendelenburg-capable beds, the entire deck tilts so the feet are higher than the head — used in certain clinical procedures.
Why the deck design matters for hip surgery patients: After hip replacement, surgeons require the hip to stay below 90 degrees of flexion. A hospital bed’s four-section deck allows the head to be raised without bending the hip — something a regular adjustable bed or recliner cannot safely do. This is one of the main clinical reasons a hospital bed is prescribed post-operatively.
The Mattress — More Medical Than You Think
A hospital bed mattress is not a regular mattress. It is a medical device in its own right. The wrong mattress on a hospital bed can cause pressure ulcers (bed sores) in as little as 2–4 hours for high-risk patients.
Types of Hospital Bed Mattresses
Standard innerspring
The most basic option. Offers firm, predictable support. Suitable for short-term recovery or patients without skin integrity concerns. Typically 6–8 inches thick to accommodate the deck’s bend points.
Foam hospital mattress
High-density medical foam conforms to the body, distributes weight more evenly, and reduces pressure points. Better than innerspring for long-term use or patients with limited mobility who can’t reposition themselves often.
Alternating pressure mattress
An active mattress system with air cells that inflate and deflate in alternating patterns, constantly redistributing pressure across the body. Clinically proven for pressure ulcer prevention. Often covered by Medicare when prescribed for wound care. This is the standard of care for high-risk patients.
Low-air-loss mattress
Similar to alternating pressure but also releases a gentle flow of air through the mattress surface, keeping skin dry and reducing moisture-related skin breakdown. Used for patients who already have existing pressure ulcers or are at very high risk. Often requires a pump unit that sits alongside the bed.
Hospital bed mattresses are sized to fit the 36″ x 80″ deck — they will not work on a standard twin bed and regular twin mattresses will not fit properly on a hospital bed.
Side rails — safety, not just a barrier
Side rails are one of the most misunderstood components of a hospital bed. Many people think of them simply as “the things that keep the patient from falling out.” They do that — but they do much more, and they need to be used correctly to avoid becoming a hazard themselves.
The two types of side rails
Full-length rails
Run the full length of the bed
Cover the entire side from head to foot. Provide maximum fall protection. However, full-length rails on both sides with a confused or restless patient can become an entrapment hazard — the patient may try to climb over or get stuck between the rail and mattress. In home settings, full-length rails require careful risk assessment.
Half-length rails
Upper or lower half only
Cover only half the bed’s length, usually positioned at the upper half (near the patient’s head and shoulders). This gives the patient a grab point for repositioning while leaving the lower half open for easier transfers in and out of bed. Half-rails are the standard recommendation for most home use situations.
What rails are actually used for
- Fall prevention: Keeps patients in the bed during sleep, especially important for patients with confusion, sedation, or neurological conditions
- Repositioning assist: Patients grab the raised rail to turn themselves, reducing the physical demand on caregivers and building patient independence
- Attachment point: Many accessories — call buttons, IV pole brackets, trapeze bars — mount directly to the side rail
- Visual boundary: Even cognitively aware patients benefit from the tactile and visual cue of where the bed ends, especially when waking disoriented at night
Important safety note on rail entrapment
The FDA has identified entrapment zones between the mattress and side rail as a patient safety risk. Always ensure the mattress fits snugly against the rail with no gap larger than 1 inch. If you notice gaps, contact your DME supplier immediately. Read the FDA’s hospital bed entrapment guidance.
Head and foot boards
The head board and foot board are the vertical panels at each end of the bed. They do more than look structural — they serve active clinical and caregiving purposes.
Head Board
- Prevents the pillow and patient from sliding toward the wall
- Provides a gripping surface for repositioning the patient from behind
- On CPR-ready beds, the head board is designed to detach quickly so a responder can kneel at the patient’s head without obstruction
- Some models allow IV poles or equipment brackets to mount to the head board
Foot Board
- Prevents the patient from sliding toward the foot of the bed
- Provides a footrest when the patient is sitting in the raised position
- Can serve as a pushing point for caregivers when maneuvering the bed
- Some foot boards include storage clips for patient charts, blankets, or small equipment
Head and foot boards on home hospital beds are generally removable — they can be detached entirely if the bed needs to be pushed against a wall or if medical access to the ends is required. On Hill-Rom and Stryker beds, the boards are engineered with quick-release mechanisms. On standard home beds, they typically slide or bolt onto the frame side rails.
Casters and wheel brakes
Hospital beds are meant to move — and to stop moving. The caster system handles both, and it is one of the most safety-critical parts of the bed.
How Casters Work
Most home hospital beds have four swivel casters — one at each corner of the base frame. Each caster rotates 360 degrees, allowing the bed to be pushed and maneuvered in any direction. On commercial hospital beds (Hill-Rom, Stryker), a fifth central caster is often added — a larger, lockable directional wheel in the center of the base frame that makes steering much easier in tight corridors.
The Brake System
Every caster has a brake pedal or lever. Pressing it down locks the wheel so the bed cannot move during patient transfers or procedures. There are two types of brake designs:
Individual Caster Brakes
Each wheel has its own brake that must be engaged separately. Common on home hospital beds. Before any patient transfer, all four brakes must be locked. This is the most important pre-transfer safety step and the most commonly skipped one.
Central Locking System
Found on commercial hospital beds. A single brake bar or lever at the foot of the bed engages all four caster brakes simultaneously. Far faster in emergency situations and reduces the risk of caregivers forgetting to lock an individual wheel.
The number one cause of bed-related falls during transfers is an unlocked caster. Always engage all wheel brakes before helping a patient get in or out of bed — every single time. It takes less than 10 seconds and prevents life-threatening injuries.
Controls and pendants — the patient’s interface
The control system is what separates a usable hospital bed from a frustrating one. Good controls give patients independence; confusing ones create dependency on caregivers for every small position change.
Patient pendant (handheld remote)
The pendant is the handheld controller that plugs into the side of the bed. It typically includes buttons for:
- Head section up and down
- Foot section up and down
- Bed height up and down (on full-electric models)
- Nurse call button (on commercial models connected to call systems)
- Control lock — prevents accidental or unauthorized adjustment
Most pendants are wired and clip to the side rail for easy reach. Some commercial models offer wireless pendants or touchscreen-based controls. The cord length matters for home use — confirm the pendant can reach the patient’s dominant hand comfortably before buying.
Side-Rail Control Panel
In addition to or instead of a pendant, many beds have a control panel built directly into the side rail. This is useful as a backup control point and for caregivers who need to adjust the bed position without reaching past the patient for the pendant.
Nurse Control Panel (foot of bed)
On commercial and semi-commercial models, a secondary control panel at the foot of the bed allows caregivers to adjust all bed functions from the foot — keeping them clear of the patient during repositioning. This panel often includes a control lockout switch that disables the patient pendant entirely, used when the patient should not self-adjust (post-surgical restrictions, fall risk).
The motor system — what makes it electric
Electric hospital beds — both semi-electric and full-electric — are powered by linear actuator motors. These are the small but powerful motors that convert electrical energy into linear (straight-line) motion, pushing and pulling the deck sections and the height mechanism.
How many motors does a hospital bed have?
Semi-electric bed
Two motors control the head section and the foot section independently. The bed’s overall height is still adjusted manually via a hand crank at the foot of the frame. This is the most common type covered by Medicare for home use.
Full-electric bed
3 or more motors
Three motors: one for head, one for foot, one for height. The patient or caregiver controls everything electrically. Advanced commercial beds may have a fourth motor for Trendelenburg tilt (full-body incline) and a fifth for lateral tilt. Full-electric is recommended for patients who need to self-reposition without assistance.
Motor safety and backup systems
All hospital bed motors are low-voltage systems (typically 24V DC) — they will not shock a patient in contact with the bed or in a wet environment. Most electric beds also include:
- Anti-entrapment logic: The motor stops if it detects resistance — preventing the deck from closing on a limb or object
- Manual backup: A manual crank or release mechanism that allows the deck to be lowered even if power is lost — critical during emergencies
- Reset button: Clears motor errors without requiring a service call — usually located under the bed frame or on the control panel
What to do if the motor stops working
First, check that the power cord is fully plugged into a working outlet. Press and hold the reset button for 5 seconds. If the motor still does not respond, check for any obstruction under the bed deck. For Hill-Rom and Stryker beds, refer to the model’s service manual or contact your DME supplier.
Common Accessories and Add-ons
The bed frame is a platform. Most hospital beds are designed to accept a range of accessories that significantly expand what the bed can do for a patient. These are the most common ones you’ll encounter:
Trapeze Bar
A triangular metal handle suspended above the patient on an overhead frame. Patients grab it to lift themselves up, shift their weight, and assist with repositioning — reducing caregiver lift demands. Essential for post-surgical patients who have upper body strength but limited leg mobility.
Overbed Table
A height-adjustable table that rolls over the bed and locks into position. Used for meals, writing, reading, or using a laptop. The table slides under the bed when not in use. Essential for patients who spend extended time in bed at home.
IV Pole
Attaches to the side rail or bed frame via a standard bracket. Holds IV bags, feeding equipment, or drainage bags at the correct height. Most home hospital beds have pre-drilled mounting holes or universal rail slots that accept standard pole brackets.
Bed Exit Alarm
A pressure sensor pad placed on the mattress under the sheet. When the patient rises and their weight leaves the pad, an alarm sounds — alerting caregivers. Invaluable for patients at fall risk, those with dementia, or anyone who might attempt to get up unsafely without assistance.
Foot Board / Foot Rest
A padded or rigid rest at the foot of the mattress. Prevents foot drop — the tendency for the foot to fall into a plantar-flexed position during extended bed rest — and provides a surface for patients to push against during exercises prescribed by physical therapists.
Transfer Board Slot
Some hospital bed side rails have a built-in slot or bracket specifically for inserting a transfer board — a smooth rigid board that the patient can slide across when moving from the bed to a wheelchair or commode chair. This significantly reduces the risk of falls during the transfer.
Need a hospital bed with the right accessories for your situation?
305 Medical Beds helps you choose the right bed, mattress, and accessories — with delivery and setup in South Florida.
Need a hospital bed with the right accessories for your situation?
305 Medical Beds helps you choose the right bed, mattress, and accessories — with delivery and setup in South Florida.Shop Hospital Beds Ask Our Team
How anatomy differs by bed type
Not every hospital bed has the same anatomy. Here is how the components differ across the most common types you’ll encounter when shopping for a home hospital bed:
Manual hospital bed
Most basic anatomy
Has all four deck sections but no motors. Head, foot, and height adjustments are all made by hand cranks located under or at the foot of the bed. Durable and low-maintenance, but requires caregiver effort for every position change. No pendant. Lowest cost — typically $500–$1,000 new. Good for short-term recovery when a caregiver is present.
Semi-electric hospital bed
2-motor anatomy
Has two motors for head and foot deck adjustment. Height is still manual. Comes with a pendant for head and foot controls. This is the most commonly Medicare-covered bed for home use — it balances convenience and cost. Most patients and caregivers find it the best all-around option for home recovery or long-term care.
Full-Electric Hospital Bed
3+ motor anatomy
All deck sections and height are motorized. Most feature-complete pendant. Best for patients who need to self-reposition without caregiver assistance — post-hip surgery, CHF, COPD, or any condition requiring frequent position changes through the night. Medicare covers full-electric only when the patient cannot operate a semi-electric model due to their medical condition.
Bariatric hospital bed
Reinforced anatomy throughout
Every structural component is upgraded — wider and heavier frame, stronger motors, wider mattress, reinforced side rails. Weight capacity starts at 600 lbs and goes up to 1,000 lbs in heavy-duty models. The deck width typically increases from 36″ to 42″–54″. All the same components as a standard bed, but built to a higher strength specification throughout.
Caring for Each Part of the Bed
A hospital bed that is well maintained lasts many years and stays safe. Each component has different care requirements — here is a simple guide organized by part:
Frame and Deck
- Wipe down with a hospital-grade disinfectant or mild soap and water after each use. Avoid abrasive cleaners that damage the powder coat.
- Inspect all deck pivot points monthly. Apply a small amount of dry lubricant (PTFE spray) if pivots squeak or feel stiff.
- Check all bolts and connection points quarterly. Vibration from motor use can loosen hardware over time.
Motors and Electrical
- Keep the motor housing clean and free of dust. Never spray liquid directly onto the motor unit.
- Inspect the power cord for damage monthly. A frayed cord on a hospital bed must be replaced immediately — do not use tape as a fix.
- Do not overextend motors — avoid holding the adjustment button once the deck has reached its travel limit. This strains the motor.
Casters
- Test all brakes weekly. A brake that feels soft or does not fully lock must be inspected before further patient use.
- Remove hair and debris from caster axles monthly — buildup can cause wheels to lock unexpectedly during bed movement.
Side Rails and Mattress
- Check all rail locking pins before every use. Rails that do not click firmly into position must be repaired before the bed is used.
- Inspect mattress cover weekly for tears. Even small tears allow moisture into the foam and create infection risk.
- Check the gap between the mattress edge and the side rail. It should never exceed 1 inch. If the mattress has compressed or shifted, reposition or replace it.
For professional servicing of any hospital bed component, contact 305 Medical Beds. We provide setup, adjustment, and service support for all beds in our inventory. For general DME maintenance resources, CMS.gov has guidelines on DME care requirements.
Still have questions about hospital bed components?
Whether you are buying, renting, or troubleshooting — our team at 305 Medical Beds is here to help. We serve South Florida with same-week delivery and hands-on setup.